Cause And Management Of Hammertoes
 Overview
Overview
Patients and doctors often refer to all forms of toe abnormalities as a Hammer toes. There are in fact four main forms of toe abnormalities, hammer toes, claw toes, mallet toes and trigger toes. A hammertoe can be best described as an abnormal contraction or "buckling" of a toe. This occurs due to a partial or complete dislocation of one of the joints that form the toe. As the toe continues to be deformed, it will press up against the shoe and may cause corns.
Causes
Claw, hammer and mallet toe are most commonly caused by wearing high heels or ill-fitting shoes that are too tight e.g. narrow toebox. If shoes like this are worn for long periods, the foot is held in a slightly bent position and gradually over time, the muscles tighten and shorten. If this continues for long enough, then the muscles become so tight that even when shoes are removed, the toe is still held in the bent position. Another common cause is Morton?s Toe, where the second toe is longer than the big toe. In this case, the second toe is commonly squashed into a shoe into an unnaturally bent position.
 Symptoms
Symptoms
People who have painful hammertoes visit their podiatrist because their affected toe is either rubbing on the end their shoe (signaling a contracted flexor tendon), rubbing on the top of their shoe (signaling a contracted extensor tendon), or rubbing on another toe and causing a painful buildup of thick skin, known as a corn.
Diagnosis
The earlier a hammertoe is diagnosed, the better the prognosis and treatment options. Your doctor will be able to diagnose your hammertoe with a simple examination of the foot and your footwear. He or she may take an x-ray to check the severity of the condition. You may also be asked about your symptoms, your normal daily activities, and your medical and family history.
Non Surgical Treatment
Wear wide shoes with plenty of room in the toes and resilient soles. Avoid wearing shoes with pointed toes. Commercially available felt pads or cushions may ease pressure from the shoe on the toe. Toe caps (small, padded sleeves that fit around the tip of the toe) may relieve the pain of hammer toe. Do toe exercises, to help toe muscles become stronger and more flexible.
Arch supports or an orthotic shoe insert prescribed by your doctor or podiatrist may help to redistribute weight on the foot. These devices do not cure the problem but may ease the symptoms of either hammer toe or mallet toe.
Surgical Treatment
Hammertoe surgery is performed when conservative measures have been exhausted and pain or deformity still persists. The surgery is performed on an outpatient basis. It typically required about one hour of time. An incision is placed over the inter-phalangeal joint. Once the bone is exposed, the end portion of the bone is removed. Your surgeon may then use pins or other fixation devices to assist in straightening the toe. These devices may be removed at a later date if necessary. Recovery for hammertoe surgery is approximately 10 to 14 days. You are hammertoe able to walk immediately following the surgery in a surgical shoe. Swelling may be present but is managed as needed. Physical therapy is used to help reduce swelling in the toe or toes after surgery. Most of these toe surgeries can be performed in the office or the outpatient surgery under local anesthesia.
 Prevention
Prevention
In addition to wearing proper shoes and socks, walking often and properly can prevent foot injury and pain. The head should be erect, the back straight, and the arms relaxed and swinging freely at the side. Step out on the heel, move forward with the weight on the outside of the foot, and complete the step by pushing off the big toe. Exercises specifically for the toe and feet are easy to perform and help strengthen them and keep them flexible. Helpful exercises include the following. Raise and curl the toes 10 times, holding each position for a count of five. Put a rubber band around both big toes and pull the feet away from each other. Count to five. Repeat 10 times. Pick up a towel with the toes. Repeat five times. Pump the foot up and down to stretch the calf and shin muscles. Perform for 2 or 3 minutes.
Bunion Hallux Valgus Surgery
Overview
 Bunion is a prominence of the medial portion of the head of the 1st metatarsal bone. The cause is often variations in position of the 1st metatarsal bone or great toe, such as lateral angulation of the great toe (hallux valgus). Secondary osteoarthritis and spur formation are common. Symptoms may include pain and redness, bursitis medial to the joint, and mild synovitis. Diagnosis is usually clinical. Treatment is usually a shoe with a wide toe box, protective pads, and orthotics. For bursitis or synovitis, corticosteroid injection may be helpful.
Bunion is a prominence of the medial portion of the head of the 1st metatarsal bone. The cause is often variations in position of the 1st metatarsal bone or great toe, such as lateral angulation of the great toe (hallux valgus). Secondary osteoarthritis and spur formation are common. Symptoms may include pain and redness, bursitis medial to the joint, and mild synovitis. Diagnosis is usually clinical. Treatment is usually a shoe with a wide toe box, protective pads, and orthotics. For bursitis or synovitis, corticosteroid injection may be helpful.
Causes
By far the most common cause of bunions is the prolonged wearing of poorly fitting shoes, usually shoes with a narrow, pointed toe box that squeezes the toes into an unnatural position. Bunions also may be caused by arthritis or polio. Heredity often plays a role in bunion formation. But these causes account for only a small percentage of bunions. A study by the American Orthopaedic Foot and Ankle Society found that 88 percent of women in the U.S. wear shoes that are too small and 55 percent have bunions. Not surprisingly, bunions are nine times more common in women than men.
Symptoms
Just because you have a bunion does not mean you will necessarily have pain. There are some people with very severe bunions and no pain and people with mild bunions and a lot of pain. Symptoms for a bunion may include pain on the inside of your foot at the big toe joint, swelling on the inside of your foot at the big toe joint, appearance of a "bump" on the inside edge of your foot. The big toe rolling over to one side. Redness on the inside of your foot at the big toe joint. Numbness or burning in the big toe (hallux). Decreased motion at the big toe joint. Painful bursa (fluid-filled sac) on the inside of your foot at the big toe joint. Pain while wearing shoes - especially shoes too narrow or with high heels. Joint pain during activities. Other conditions which may appear with bunions include Corns in between the big toe and second toe. Callous formation on the side or bottom of the big toe or big toe joint. Callous under the second toe joint. Pain in the second toe joint.
Diagnosis
X-rays are the best way to determine the amount of deformity of the MTP joint. Blood work may be required to rule out other diseases that may be associated with bunions such as rheumatoid arthritis. Other tests such as bone scans or MRI's are not usually required.
Non Surgical Treatment
Wearing the right shoes, using shoe inserts (orthoses) and padding, and taking painkillers can all help to ease your symptoms of a bunion. However, these treatments can?t cure a bunion or stop it getting worse. If you have severe pain or discomfort from a bunion, you may be advised to have an operation to correct it. One of the most important things you can do is to wear the right footwear. You should try to wear flat, wide-fitting shoes with laces or an adjustable strap that fits you properly. You may also want to place a bunion pad over your bunion to give it some protection from the pressure of your shoes. You can usually buy these pads from a pharmacy, or get them from your podiatrist or chiropodist. He or she may also recommend a shoe insert, which can be moulded specifically to your foot. Shoe inserts aim to reduce the pain of your bunion by improving how you walk. You can take over-the-counter painkillers, such as paracetamol or ibuprofen, to help relieve the pain and inflammation of your bunion. Always follow the instructions in the patient information leaflet that comes with your medicine. Medicines give temporary relief but they won?t be able to cure your bunion or prevent it from getting worse. If you have a bunion as a result of underlying arthritis, your doctor may prescribe specific medicines to treat this. 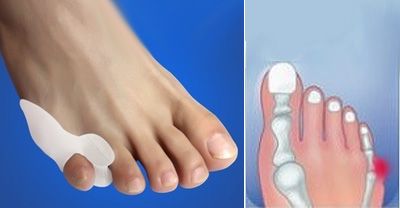
Surgical Treatment
Bunion surgery is most often done on an outpatient or day-surgery basis, usually with a local anesthetic technique called an ankle block. The surgery typically takes an hour or two to perform. Following your surgery, you will stay in the Recovery Room for several hours while the anesthetic wears off. For your safety, you will be required to have someone to drive you home. You should keep in mind that any surgery carries with it very small-but-possible risks of complications such as allergic reaction to anesthesia, bleeding and infection.
What Are The Causes And Signals Of A Ruptured Achilles Tendon?
Overview
 The Achilles tendon is a conjoined tendon composed of the gastrocnemius and soleus muscles with occasional contribution from the plantaris muscle, and it inserts on the calcaneal tuberosity. The plantaris muscle is absent in 6% to 8% of individuals. The Achilles tendon is approximately 15-cm long and is the largest and strongest tendon in the human body. The tendon spirals approximately 90? from its origin to its insertion and this twisting produces an area of stress approximately 2- to 5-cm proximal to its insertion. The tendon has no true synovial sheath; instead it is wrapped in a paratenon. The Achilles tendon experiences the highest loads of any tendon in the body, and bears tensile loads up to 10 times body weight during athletic activities. The tendon most commonly ruptures in a region 2- to 6-cm proximal to its insertion.
The Achilles tendon is a conjoined tendon composed of the gastrocnemius and soleus muscles with occasional contribution from the plantaris muscle, and it inserts on the calcaneal tuberosity. The plantaris muscle is absent in 6% to 8% of individuals. The Achilles tendon is approximately 15-cm long and is the largest and strongest tendon in the human body. The tendon spirals approximately 90? from its origin to its insertion and this twisting produces an area of stress approximately 2- to 5-cm proximal to its insertion. The tendon has no true synovial sheath; instead it is wrapped in a paratenon. The Achilles tendon experiences the highest loads of any tendon in the body, and bears tensile loads up to 10 times body weight during athletic activities. The tendon most commonly ruptures in a region 2- to 6-cm proximal to its insertion.
Causes
As with any muscle or tendon in the body, the Achilles tendon can be torn if there is a high force or stress on it. This can happen with activities which involve a forceful push off with the foot, for example, in football, running, basketball, diving, and tennis. The push off movement uses a strong contraction of the calf muscles which can stress the Achilles tendon too much. The Achilles tendon can also be damaged by injuries such as falls, if the foot is suddenly forced into an upward-pointing position, this movement stretches the tendon. Another possible injury is a deep cut at the back of the ankle, which might go into the tendon. Sometimes the Achilles tendon is weak, making it more prone to rupture. Factors that weaken the Achilles tendon are as follows. Corticosteroid medication (such as prednisolone) - mainly if it is used as long-term treatment rather than a short course. Corticosteroid injection near the Achilles tendon. Certain rare medical conditions, such as Cushing's syndrome, where the body makes too much of its own corticosteroid hormones. Increasing age. Tendonitis (inflammation) of the Achilles tendon. Other medical conditions which can make the tendon more prone to rupture; for example, rheumatoid arthritis, gout and systemic lupus erythematosus (SLE), lupus. Certain antibiotic medicines may slightly increase the risk of having an Achilles tendon rupture. These are the quinolone antibiotics such as ciprofloxacin and ofloxacin. The risk of having an Achilles tendon rupture with these antibiotics is actually very low, and mainly applies if you are also taking corticosteroid medication or are over the age of about 60.
Symptoms
Patients who suffer an acute rupture of the Achilles tendon often report hearing a ?pop?or ?snap.? Patients usually have severe pain the back of the lower leg near the heel. This may or may not be accompanied by swelling. Additionally, because the function of the Achilles tendon is to enable plantarflexion (bending the foot downward), patients often have difficulty walking or standing up on their toes. With a complete rupture of the tendon, the foot will not move. In cases where the diagnosis is equivocal, your physician may order an MRI of the leg to diagnose a rupture of the Achilles tendon.
Diagnosis
The diagnosis of an Achilles tendon rupture can be made easily by an orthopedic surgeon. The defect in the tendon is easy to see and to palpate. No x-ray, MRI or other tests are necessary.
Non Surgical Treatment
Initial treatment for sprains and strains should occur as soon as possible. Remember RICE! Rest the injured part. Pain is the body's signal to not move an injury. Ice the injury. This will limit the swelling and help with the spasm. Compress the injured area. This again, limits the swelling. Be careful not to apply a wrap so tightly that it might act as a tourniquet and cut off the blood supply. Elevate the injured part. This lets gravity help reduce the swelling by allowing fluid and blood to drain downhill to the heart. Over-the-counter pain medication is an option. Acetaminophen (Tylenol) is helpful for pain, but ibuprofen (Motrin, Advil, Nuprin) might be better, because these medications relieve both pain and inflammation. Remember to follow the guidelines on the bottle for appropriate amounts of medicine, especially for children and teens. 
Surgical Treatment
Operative treatment involves a 6cm incision along the inner side of the tendon. The torn ends are then strongly stitched together with the correct tension. After the operation a below knee half cast is applied for 2 weeks. At 2 weeks a brace will be applied that will allow you to move the foot and fully weight-bear for a further 6 weeks. After this you will need physiotherapy. Surgery carries the general risks of any operation but the risk of re-rupture is greatly reduced to 2%. The best form of treatment is controversial with good results being obtained by both methods but surgery is generally recommended for patients under 60 years of age who are fit and active with an intra-substance tear.
Prevention
You can help to reduce your risk of an injury to your Achilles tendon by doing the following. When you start a new exercise regime, gradually increase the intensity and the length of time you spend being active. Warm up your muscles before you exercise and cool them down after you have finished. The benefit of stretching before or after exercise is unproven. However, it may help to stretch your calf muscles, which will help to lengthen your Achilles tendon, before you exercise. Wear appropriate and well-fitting shoes when you exercise.